




Zahin Amin-Chowdhury
@acciochoc.bsky.social
epidemiologist @UKHSA • MSc Epi @lshtm • excited about all things #infectiousdiseases #vaccines #pneumococcus & now #hcai
👏 finally appreciation for the huge team effort contributing to this report & surveillance - from the healthcare staff at NHS acute trusts who are submitting the data on regular basis, to the epidemiologists crunching the data & everyone providing input.
September 26, 2025 at 9:46 PM
👏 finally appreciation for the huge team effort contributing to this report & surveillance - from the healthcare staff at NHS acute trusts who are submitting the data on regular basis, to the epidemiologists crunching the data & everyone providing input.
📊 Mortality
• 30-day case-fatality rate (CFR) fell or stayed stable (except MSSA ↑ 5.2%).
• 30-day mortality rate rose for most infections (in line with incidence rises).
• Graph ⬇️ with data up to 2022/23 shows CFRs across the infections - P. aeruginosa & MRSA among highest CFRs (23-26%)
• 30-day case-fatality rate (CFR) fell or stayed stable (except MSSA ↑ 5.2%).
• 30-day mortality rate rose for most infections (in line with incidence rises).
• Graph ⬇️ with data up to 2022/23 shows CFRs across the infections - P. aeruginosa & MRSA among highest CFRs (23-26%)

September 26, 2025 at 9:46 PM
📊 Mortality
• 30-day case-fatality rate (CFR) fell or stayed stable (except MSSA ↑ 5.2%).
• 30-day mortality rate rose for most infections (in line with incidence rises).
• Graph ⬇️ with data up to 2022/23 shows CFRs across the infections - P. aeruginosa & MRSA among highest CFRs (23-26%)
• 30-day case-fatality rate (CFR) fell or stayed stable (except MSSA ↑ 5.2%).
• 30-day mortality rate rose for most infections (in line with incidence rises).
• Graph ⬇️ with data up to 2022/23 shows CFRs across the infections - P. aeruginosa & MRSA among highest CFRs (23-26%)
More on these health inequalities in this research article by @andmazzella.bsky.social et al.
Health inequalities in incidence of bacteraemias: a national surveillance and data linkage study, England, 2018 to 2022
Background Health inequalities exist globally, but limited data exist on this topic for bacteraemia. Aim In this study we investigated health inequalities surrounding bacteraemia in England, to identify high-risk population groups and areas of intervention. Methods We retrospectively analysed English surveillance data between 2018 and 2022 for Escherichia coli, Klebsiella species, Pseudomonas aeruginosa, and both meticillin-sensitive and resistant Staphylococcus aureus (MSSA, MRSA) bacteraemia. Crude incidence rates stratified by index of multiple deprivation and ethnic groups were calculated; age-adjusted rate ratios were estimated using negative binomial regression models. Results We identified 342,787 bacteraemia cases. Across all pathogens, as the level of deprivation rose, so did the age-adjusted bacteraemia incidence rate ratio. Compared with residents of the 20% least deprived areas of England, residents of the 20% most deprived areas had a 2.68-fold increased bacteraemia rate for MRSA (95% CI: 2.29–3.13) and 1.95-fold for E. coli (95% CI: 1.84–2.05), and 15% higher odds of dying within 30 days of any bacteraemia (95% CI: 1.13–1.19). After age adjustment, the incidence of all bacteraemia was higher in the Asian and Black groups compared with the White group: for MRSA, 79% higher in the Asian (95% CI: 1.51–2.10) and 59% higher in the Black (95% CI: 1.29–1.95) groups. The exception was MSSA, whose incidence was highest in the White group. Conclusion Disproportionately higher age-adjusted incidence of bacteraemia occurred in deprived areas and ethnic minorities. These disparities are likely multifactorial, possibly including socioeconomic, cultural, and systemic risk factors and different burden of comorbidities. Better understanding these factors can enable targeted interventions.
www.eurosurveillance.org
September 26, 2025 at 9:46 PM
More on these health inequalities in this research article by @andmazzella.bsky.social et al.
⚖️ Ethnicity & deprivation
• Black & Asian groups show the highest age-standardised incidence for most infections (except CDI → highest remained in White group).
• Deprivation: the most deprived areas had 1.5-3.1x higher age-sex standardised incidence vs least deprived.
• Black & Asian groups show the highest age-standardised incidence for most infections (except CDI → highest remained in White group).
• Deprivation: the most deprived areas had 1.5-3.1x higher age-sex standardised incidence vs least deprived.
September 26, 2025 at 9:46 PM
⚖️ Ethnicity & deprivation
• Black & Asian groups show the highest age-standardised incidence for most infections (except CDI → highest remained in White group).
• Deprivation: the most deprived areas had 1.5-3.1x higher age-sex standardised incidence vs least deprived.
• Black & Asian groups show the highest age-standardised incidence for most infections (except CDI → highest remained in White group).
• Deprivation: the most deprived areas had 1.5-3.1x higher age-sex standardised incidence vs least deprived.
Clostridioides difficile infections
⚠️ ↑ ~50% since 2020/21 to 33.3 per 100k – the highest since 2011/12. Driven by both hospital- and community-onset cases.
See more on recent CDI rises in this technical report:
⚠️ ↑ ~50% since 2020/21 to 33.3 per 100k – the highest since 2011/12. Driven by both hospital- and community-onset cases.
See more on recent CDI rises in this technical report:

Increase in Clostridioides difficile infections (CDI): current epidemiology, data and investigations – Technical report
www.gov.uk
September 26, 2025 at 9:46 PM
Clostridioides difficile infections
⚠️ ↑ ~50% since 2020/21 to 33.3 per 100k – the highest since 2011/12. Driven by both hospital- and community-onset cases.
See more on recent CDI rises in this technical report:
⚠️ ↑ ~50% since 2020/21 to 33.3 per 100k – the highest since 2011/12. Driven by both hospital- and community-onset cases.
See more on recent CDI rises in this technical report:
MSSA bacteraemia
↗️ Year-on-year increases continue following the pandemic dip (similar to E. coli), reaching ↑ 12% (unlike E. coli) pre-pandemic levels at 24.2 per 100k.
Community-onset cases were the main driver.
↗️ Year-on-year increases continue following the pandemic dip (similar to E. coli), reaching ↑ 12% (unlike E. coli) pre-pandemic levels at 24.2 per 100k.
Community-onset cases were the main driver.

September 26, 2025 at 9:46 PM
MSSA bacteraemia
↗️ Year-on-year increases continue following the pandemic dip (similar to E. coli), reaching ↑ 12% (unlike E. coli) pre-pandemic levels at 24.2 per 100k.
Community-onset cases were the main driver.
↗️ Year-on-year increases continue following the pandemic dip (similar to E. coli), reaching ↑ 12% (unlike E. coli) pre-pandemic levels at 24.2 per 100k.
Community-onset cases were the main driver.
MRSA bacteraemia
⚠️ Sharp ↑ 29.5% to 1.9 per 100k vs 2018/19. Reaching a 12-year high & biggest annual increase since surveillance began. Both hospital- and community-onset driving the rise.
⚠️ Sharp ↑ 29.5% to 1.9 per 100k vs 2018/19. Reaching a 12-year high & biggest annual increase since surveillance began. Both hospital- and community-onset driving the rise.

September 26, 2025 at 9:46 PM
MRSA bacteraemia
⚠️ Sharp ↑ 29.5% to 1.9 per 100k vs 2018/19. Reaching a 12-year high & biggest annual increase since surveillance began. Both hospital- and community-onset driving the rise.
⚠️ Sharp ↑ 29.5% to 1.9 per 100k vs 2018/19. Reaching a 12-year high & biggest annual increase since surveillance began. Both hospital- and community-onset driving the rise.
Pseudomonas aeruginosa bacteraemia
↔️ Incidence has mostly remained steady → 7.8 per 100k in 2024/25.
🏥 Hospital-onset incidence = 4.8 per 100k bed-days.
↔️ Incidence has mostly remained steady → 7.8 per 100k in 2024/25.
🏥 Hospital-onset incidence = 4.8 per 100k bed-days.

September 26, 2025 at 9:46 PM
Pseudomonas aeruginosa bacteraemia
↔️ Incidence has mostly remained steady → 7.8 per 100k in 2024/25.
🏥 Hospital-onset incidence = 4.8 per 100k bed-days.
↔️ Incidence has mostly remained steady → 7.8 per 100k in 2024/25.
🏥 Hospital-onset incidence = 4.8 per 100k bed-days.
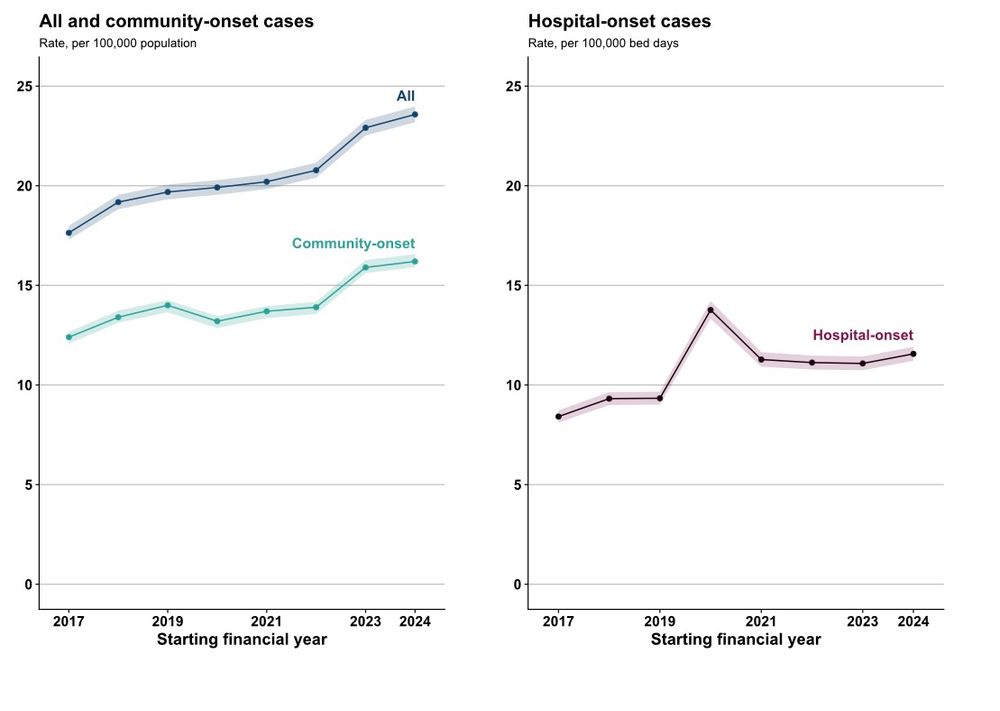
Klebsiella spp. bacteraemia
↗️ Last year saw the sharpest increase since surveillance began - ↑ 10.3%.
Incidence rose again this year to 23.6 per 100k (+2.9% vs 2023/24).
Largely driven by community-onset infections. While most age-sex groups saw rise, particularly notable among male 75+ years.
↗️ Last year saw the sharpest increase since surveillance began - ↑ 10.3%.
Incidence rose again this year to 23.6 per 100k (+2.9% vs 2023/24).
Largely driven by community-onset infections. While most age-sex groups saw rise, particularly notable among male 75+ years.
September 26, 2025 at 9:46 PM
Klebsiella spp. bacteraemia
↗️ Last year saw the sharpest increase since surveillance began - ↑ 10.3%.
Incidence rose again this year to 23.6 per 100k (+2.9% vs 2023/24).
Largely driven by community-onset infections. While most age-sex groups saw rise, particularly notable among male 75+ years.
↗️ Last year saw the sharpest increase since surveillance began - ↑ 10.3%.
Incidence rose again this year to 23.6 per 100k (+2.9% vs 2023/24).
Largely driven by community-onset infections. While most age-sex groups saw rise, particularly notable among male 75+ years.
E. coli bacteraemia
⤴️ In 2024/25, cases rose 17% since 2020/21 → 76.6 per 100k. This rise follows the COVID-19 pandemic dip and is now back to levels similar to those seen in 2018/19.
Most (81%) remain community-onset.
⤴️ In 2024/25, cases rose 17% since 2020/21 → 76.6 per 100k. This rise follows the COVID-19 pandemic dip and is now back to levels similar to those seen in 2018/19.
Most (81%) remain community-onset.

September 26, 2025 at 9:46 PM
E. coli bacteraemia
⤴️ In 2024/25, cases rose 17% since 2020/21 → 76.6 per 100k. This rise follows the COVID-19 pandemic dip and is now back to levels similar to those seen in 2018/19.
Most (81%) remain community-onset.
⤴️ In 2024/25, cases rose 17% since 2020/21 → 76.6 per 100k. This rise follows the COVID-19 pandemic dip and is now back to levels similar to those seen in 2018/19.
Most (81%) remain community-onset.
Reposted by Zahin Amin-Chowdhury

The big question is: why do we see these sad inequalities?
Difficult to say: complex intersection of factors.
People living in more deprived areas and certain ethnic minorities tend to be more affected by:
💔 predisposing comorbidities
💸 poverty
🏫 low educational attainment
⚕️barriers to healthcare
Difficult to say: complex intersection of factors.
People living in more deprived areas and certain ethnic minorities tend to be more affected by:
💔 predisposing comorbidities
💸 poverty
🏫 low educational attainment
⚕️barriers to healthcare
March 6, 2025 at 5:33 PM
The big question is: why do we see these sad inequalities?
Difficult to say: complex intersection of factors.
People living in more deprived areas and certain ethnic minorities tend to be more affected by:
💔 predisposing comorbidities
💸 poverty
🏫 low educational attainment
⚕️barriers to healthcare
Difficult to say: complex intersection of factors.
People living in more deprived areas and certain ethnic minorities tend to be more affected by:
💔 predisposing comorbidities
💸 poverty
🏫 low educational attainment
⚕️barriers to healthcare
Hope your 3 o’clock meeting didn’t push you over the edge 🙃
December 4, 2024 at 9:28 PM
Hope your 3 o’clock meeting didn’t push you over the edge 🙃